The clinical and radiological findings of thyroid eye disease — eye signs, orbital CT, disease-activity scoring (CAS), and severity grading.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
Part of our complete guide to Thyroid Eye Disease (TED) — this page covers TED diagnosis and evaluation in depth.
Thyroid eye disease is recognized by a characteristic set of eye findings and graded by how active and how severe it is. This page covers the clinical signs, the orbital imaging, and the scoring systems used to guide treatment.

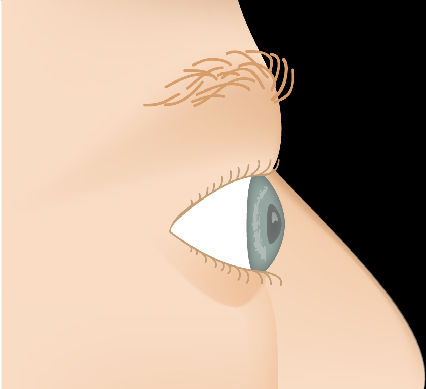
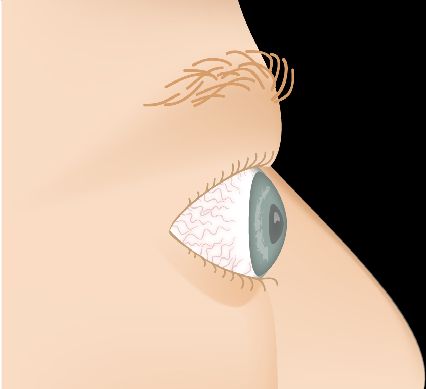
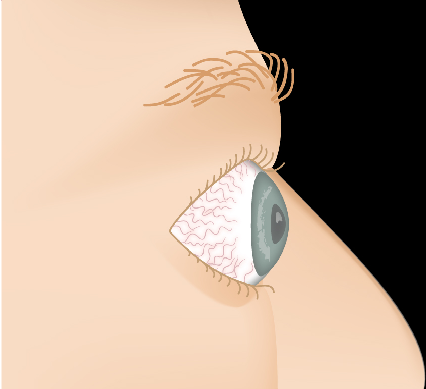
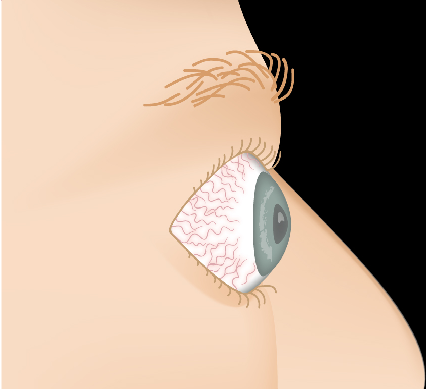
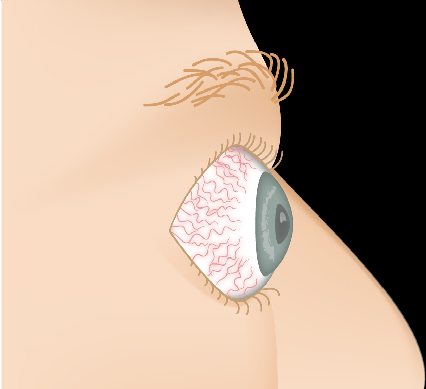
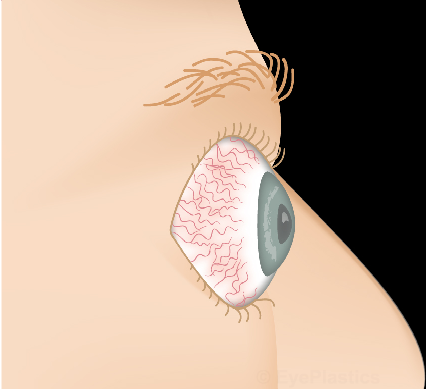
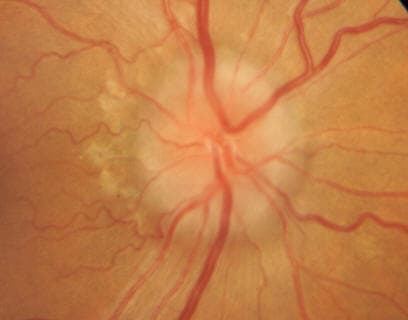
The hallmark findings of TED include proptosis, lid retraction, restricted eye movement, and periorbital swelling. The combination of these features gives the characteristic “staring” or “startled” appearance.



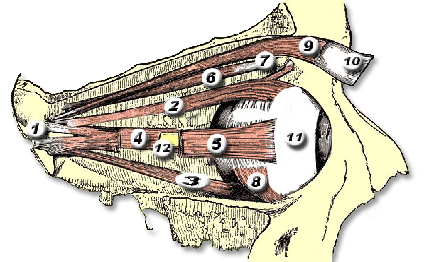
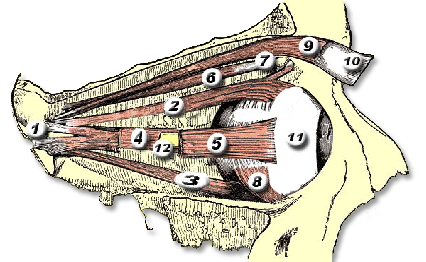
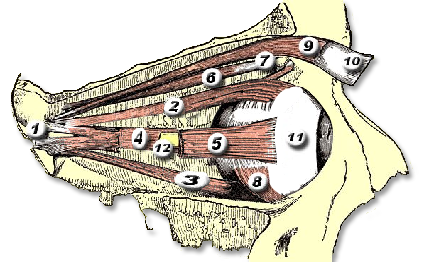
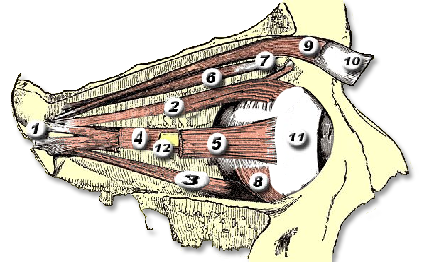
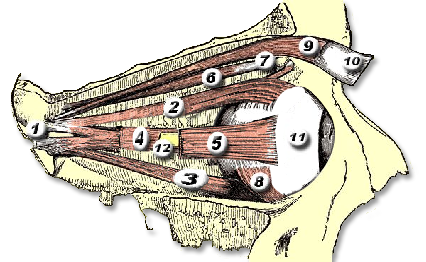
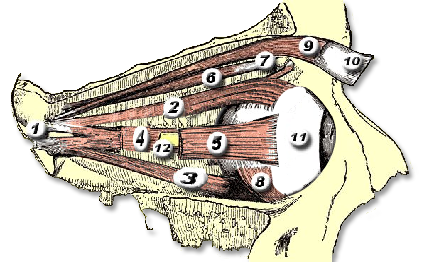
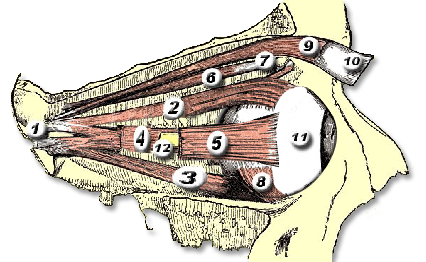
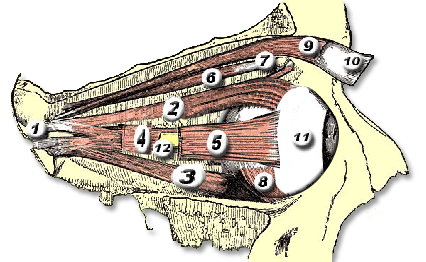
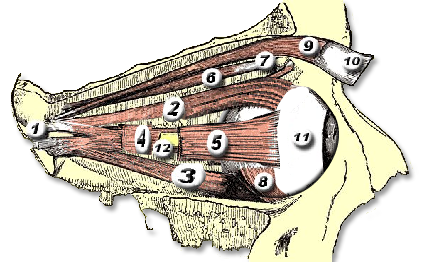
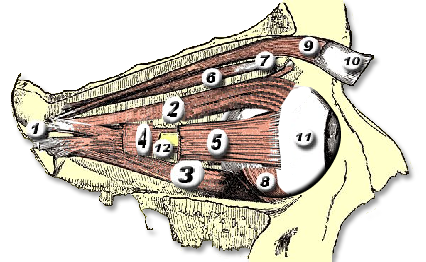
Interactive visualization showing orbital muscle changes and progressive proptosis associated with Thyroid Eye Disease.
Drag the slider to compare


CT of the orbits characteristically demonstrates enlarged extraocular muscles (particularly inferior and medial rectus) with sparing of the tendinous insertions — a key feature distinguishing TED from orbital myositis, where the tendon is involved. Crowding of the enlarged muscles at the orbital apex (apical crowding) predicts risk of optic neuropathy.
TED has two distinct phases: an active (inflammatory) phase of variable duration (typically 6–24 months) followed by an inactive (fibrotic) phase. Timing of treatment is critical — most medical therapies work only during the active phase.
The CAS assigns one point for each of the following signs of active inflammation:
A CAS ≥ 3/7 indicates active disease. Active disease may respond to medical therapy such as corticosteroids and the IGF-1R inhibitor teprotumumab (Tepezza); teprotumumab requires monitoring for hearing impairment and hyperglycemia; it can harm a developing fetus, so it must not be used in pregnancy and effective contraception is required during treatment and for 6 months after the final dose; inactive disease does not — surgical rehabilitation is the appropriate approach for stable inactive TED.
Sight-threatening TED: Compressive optic neuropathy or severe corneal exposure requires urgent treatment — urgent high-dose IV corticosteroids and/or orbital decompression surgery regardless of disease phase. Any sudden decrease in vision, dimming of color, or severe eye pain warrants same-day emergency evaluation.

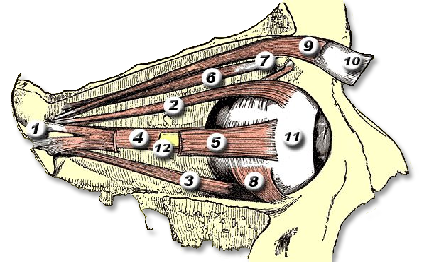
In TED, the extraocular muscles become infiltrated with inflammatory cells, expand due to glycosaminoglycan deposition, and eventually fibrosis. The inferior and medial rectus muscles are most consistently affected, producing the characteristic upward and outward gaze restrictions and diplopia.
| Muscle | Primary Function | TED Involvement |
|---|---|---|
| Inferior rectus | Depression (downgaze) | Most commonly enlarged — causes hypotropia and limited upgaze; compresses optic nerve at apex |
| Medial rectus | Adduction | Second most affected — causes esotropia and limited abduction; diplopia on lateral gaze |
| Superior rectus / levator | Elevation / lid opening | Enlargement restricts downgaze; levator fibrosis and sympathetic Müller muscle stimulation cause lid retraction |
| Lateral rectus | Abduction | Less commonly enlarged |
| Superior oblique | Intorsion / depression | Rarely affected |
For detailed orbital bone and muscle anatomy, see our Anatomy Overview page.
Connect with a board-certified oculoplastic surgeon who specializes in thyroid eye disease: signs, symptoms & diagnosis.
Search the Directory →