Surgery that enlarges the bony orbit to relieve proptosis and optic-nerve compression in thyroid eye disease — the first step of rehabilitative surgery.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
Part of our complete guide to Thyroid Eye Disease (TED) — this page covers orbital decompression surgery in depth.
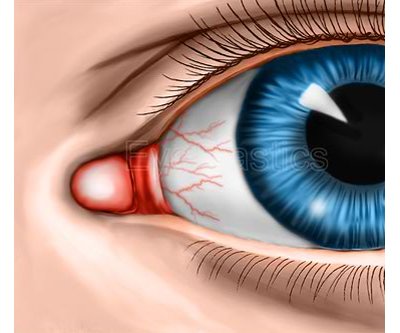
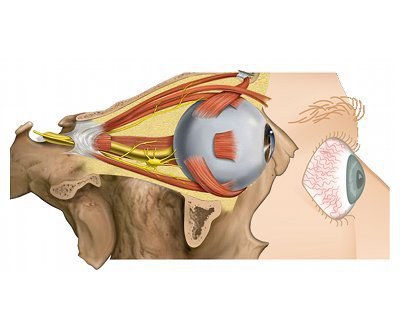
Orbital decompression is the first and most fundamental of the rehabilitative operations for thyroid eye disease. By enlarging the bony eye socket it relieves a bulging eye and, when needed, pressure on the optic nerve.
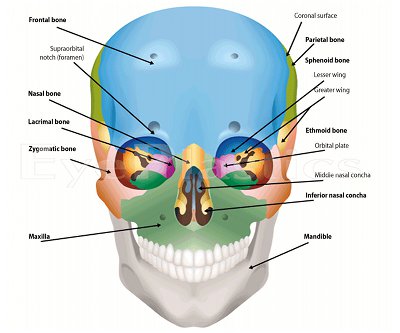
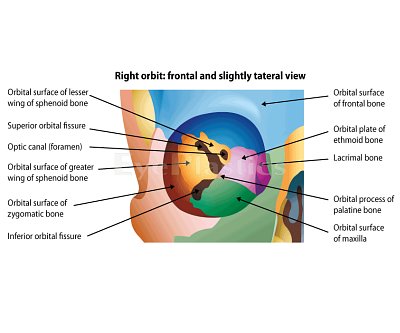
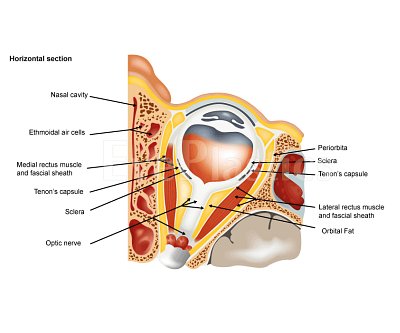
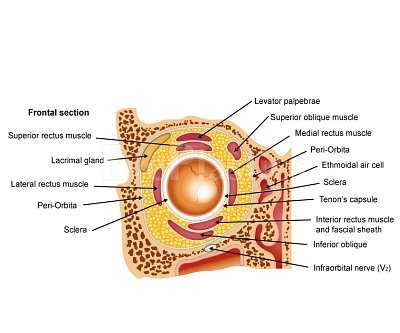
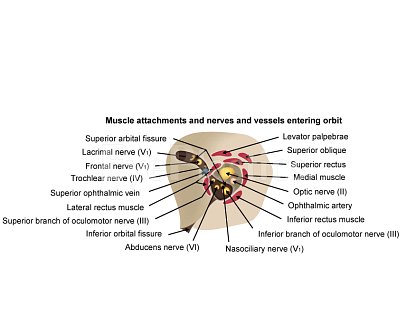
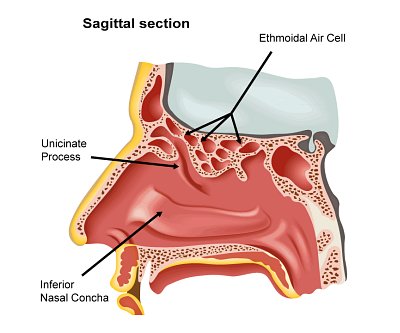
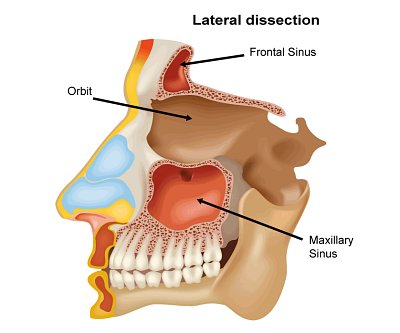
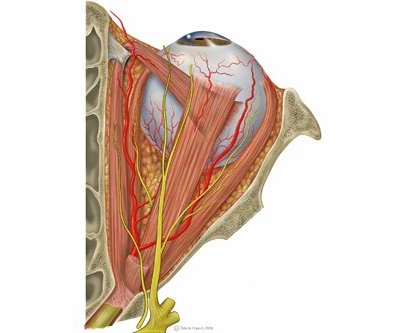
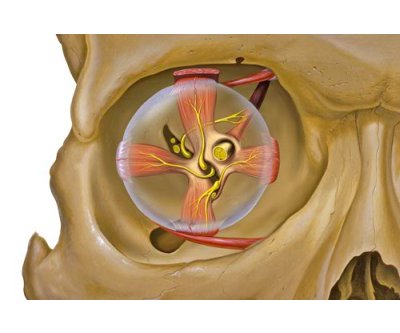
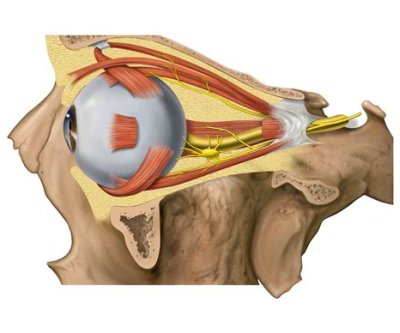
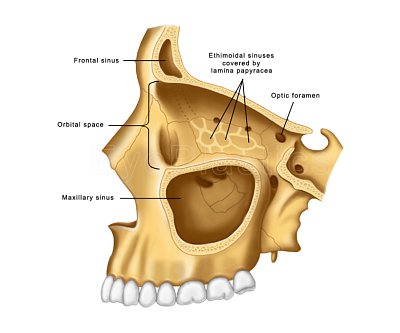
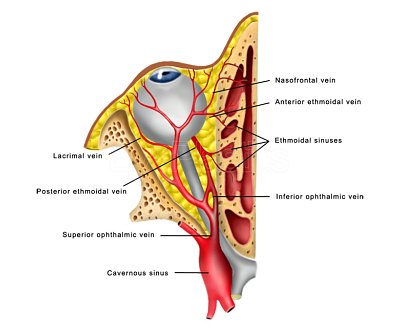
Explore orbital anatomy, clinical findings, and the medial wall, lateral wall, and floor decompression surgical techniques.
Choose a section, then drag the slider to step through it.
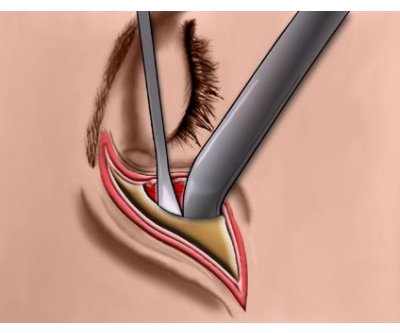
Step 1 of 14
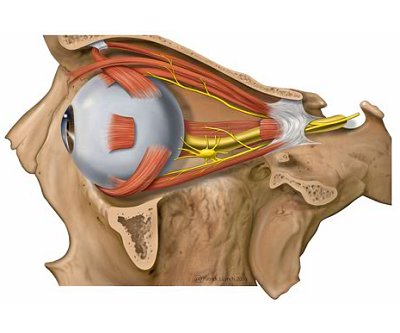
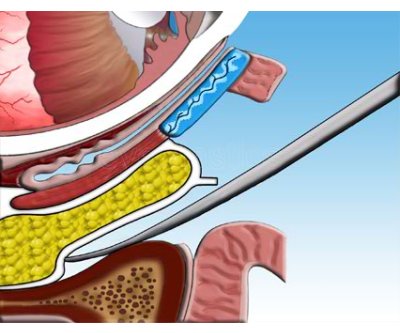
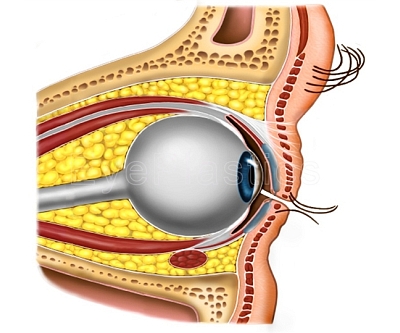
In order to create additional space on the outer orbit, the surgeon may remove some of this bone with (as seen here) or thin the bone in this area.
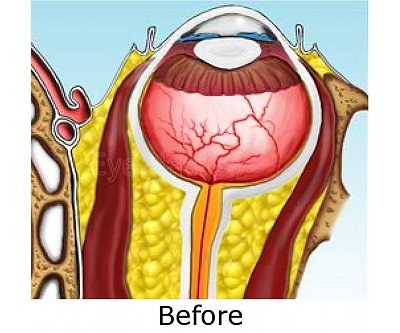
Drag the slider to compare
Orbital decompression creates additional volume within the orbit by removing one or more orbital walls, allowing the expanded orbital contents to bulge into the adjacent sinuses. This reduces proptosis, relieves corneal exposure, and — crucially — decompresses the optic nerve when vision is threatened.
Your oculoplastic surgeon tailors the approach to each patient’s CT anatomy, severity, and goals:
Connect with a board-certified oculoplastic surgeon who specializes in orbital decompression surgery.
Search the Directory →