Chronic infection of the tear-drainage canaliculus — most often from Actinomyces concretions — presenting as a red, “pouting” punctum with one-sided discharge. Definitive cure is removal of the concretions by canaliculotomy and curettage.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
Part of our complete guide to Tear-Duct & Lacrimal Surgery — this page covers canaliculitis in depth.
Canaliculitis is a chronic infection of the canaliculus — one of the two narrow channels that carry tears from the puncta (the tiny openings at the inner corner of each eyelid) toward the lacrimal sac. Although uncommon, it is one of the most frequently missed diagnoses in oculoplastic practice: because it mimics ordinary conjunctivitis, patients are often treated for a persistent, one-sided “pink eye” for months or even years before the true cause is recognized.

Canaliculitis vs. dacryocystitis. Both cause a red, watery, discharging eye, but the location of the swelling separates them. Canaliculitis is centered at the punctum and canaliculus, above the medial canthal tendon. Dacryocystitis — infection of the tear sac — produces a tender bulge below the tendon. Getting this distinction right changes the entire treatment plan.
Canaliculitis is most often caused by Actinomyces israelii, a slow-growing, filamentous, gram-positive bacterium that grows under anaerobic to microaerophilic conditions. Inside the canaliculus the organism aggregates into firm yellowish concretions (canalicular dacryoliths, classically described as “sulfur granules”). These concretions are the engine of the disease: they shelter bacteria from tears and topical drops, which is why the infection smolders and relapses until the concretions themselves are physically removed.
A common trigger: punctal and canalicular plugs. Plugs and intracanalicular implants placed for dry eye — and retained lacrimal stents — are a well-recognized cause of canaliculitis, because they create a foreign-body surface for bacteria to colonize. Any patient with a plug who develops a chronically red, discharging eye should be evaluated for canaliculitis. The condition is also seen most often in middle-aged and older adults, and somewhat more frequently in women.
The classic presentation is a triad of chronic one-sided tearing, discharge, and a red, swollen punctum. The single most useful sign is the “pouting punctum” — a dilated, erythematous, everted punctum that looks pushed open by the material within the canaliculus.

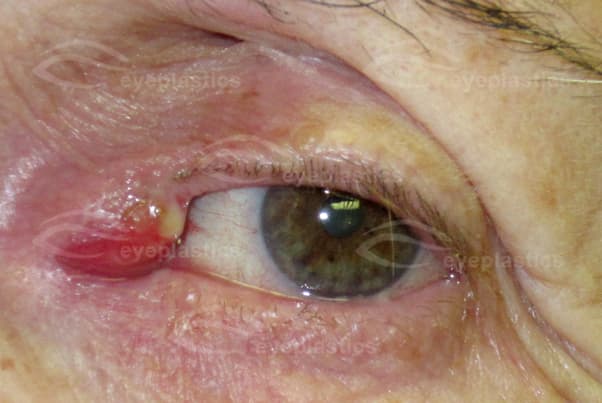
Canaliculitis is a clinical diagnosis. The combination of a pouting punctum, localized canalicular swelling, and expressible concretions is highly specific. Gentle pressure over the canaliculus that produces granular discharge essentially confirms it at the slit lamp.
The guiding principle is simple: the concretions must be physically removed. Antibiotic drops alone — the most common initial treatment — usually fail, because the medication cannot penetrate the concretions that harbor the bacteria. Definitive cure comes from clearing the canaliculus.
Warm compresses, canalicular massage to express material, and topical or irrigated antibiotics (penicillin G is highly effective against Actinomyces) may temporarily improve symptoms and are useful adjuncts, but they rarely cure the disease on their own.
The most effective and lowest-recurrence treatment is a canaliculotomy: a small linear incision made along the conjunctival (inner) surface of the canaliculus to open it, followed by thorough curettage to remove every concretion. The canaliculus is then irrigated with antibiotic solution. Performed through the back surface of the eyelid, it leaves no visible external scar.
The main long-term concern is canalicular scarring or narrowing (stenosis) after surgery, which can itself cause tearing. Careful, canaliculus-sparing technique — and, in selected cases, temporary stenting — minimizes this risk. Prognosis is excellent once the concretions are fully cleared.
Canaliculitis is one part of a larger group of tear-drainage problems. For the related infection of the tear sac and for canalicular-laceration repair, see Tear-Sac Infections & Lacrimal Trauma; for blocked tear ducts and DCR surgery, see Blocked Tear Duct & DCR; and for the broader picture of periocular infection, see the Infections overview.
Connect with a board-certified oculoplastic surgeon who specializes in canaliculitis.
Search the Directory →