Acquired nasolacrimal duct obstruction and its surgical treatment — dacryocystorhinostomy (DCR), probing, and silicone intubation.
Medically reviewed by EyePlastics Medical Editorial Board·ASOPRS oculoplastic surgeons·Last updated June 2026
Explore lacrimal anatomy and surgical treatments including probing, silicone intubation, DCR, and CDCR using the menu on the left.
Lacrimal SystemInteractive Surgical Animation
Choose a procedure, then drag the slider to step through it.
Step 1 of 7
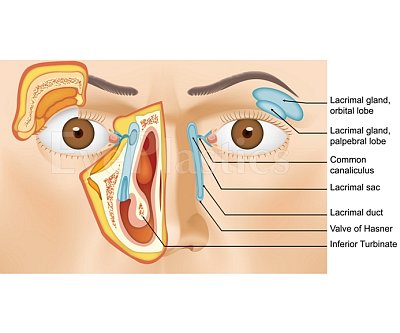
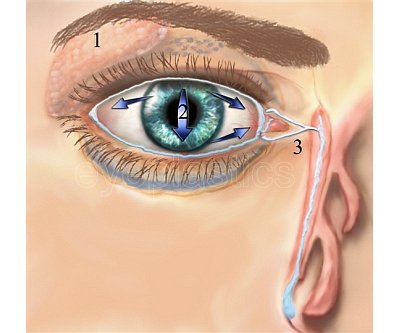
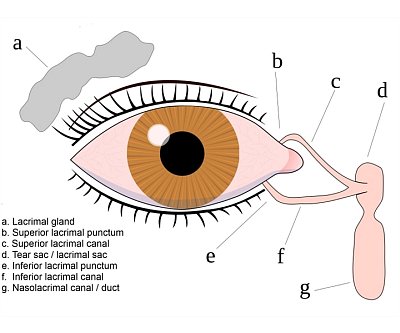
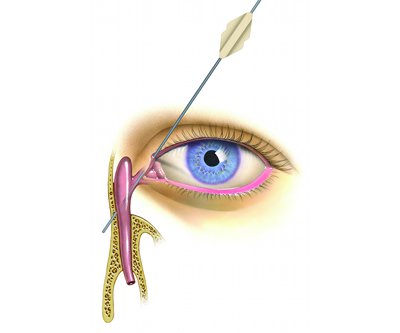
Anatomical drawing of the tear duct (lacrimal system). The lacrimal gland produces the majority of the tears. The lacrimal duct drains the tears.
DCR surgery may performed with the aid of a special endoscope to look up the nose (Endoscopic DCR).
DCR surgery may performed with the aid of a special endoscope to look up the nose (Endoscopic DCR).
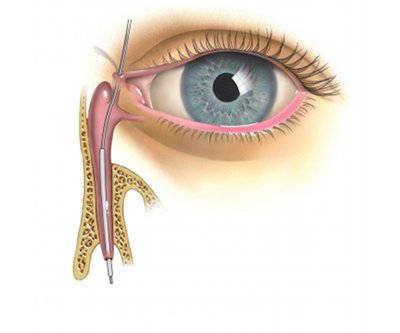
A new bypass channel is created between the lacrimal sac and nasal cavity and then connecting the lacrimal sac to the lining of the inside of the nose. Silicone stents are placed in this pathway.
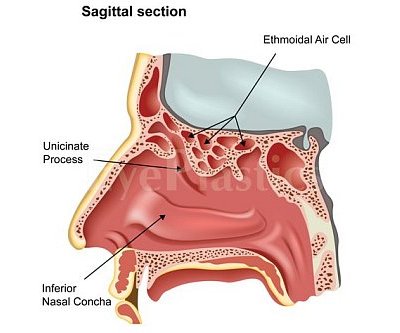
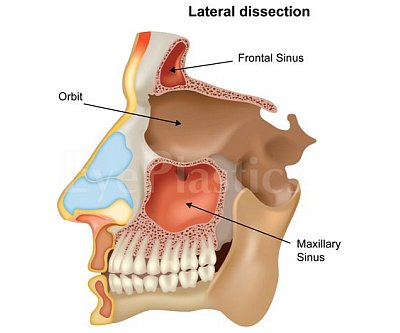
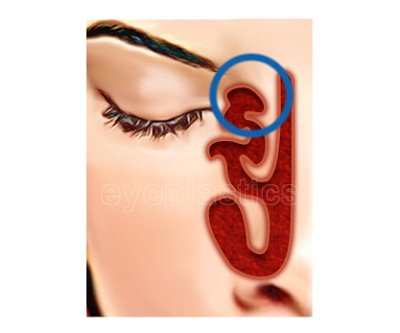
This illustrates the sinuses and orbital components.
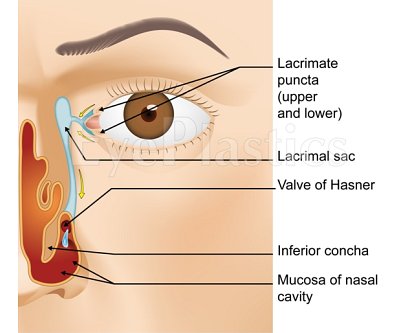
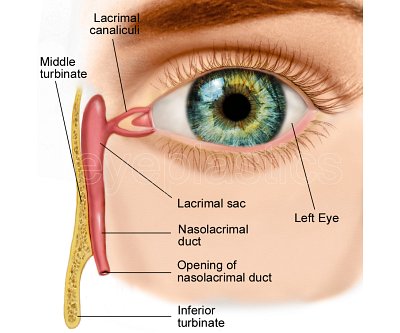
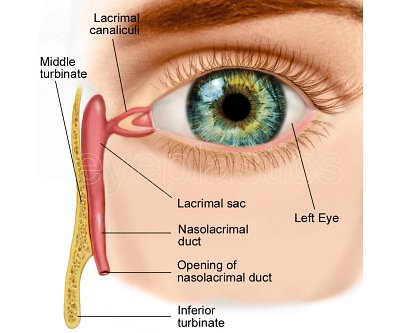
Labeled illustration of the various components of the lacrimal system.
Anatomical drawing of the tear duct (lacrimal system).
Drag the slider to compare
Part of our complete guide to Tear-Duct & Lacrimal Surgery — this page covers blocked tear ducts and DCR surgery in depth.
When tears cannot drain, they overflow onto the cheek and the tear sac can become a reservoir for infection. A blocked nasolacrimal duct is the most common cause, and the definitive fix is surgery to restore drainage. The animation below walks through probing, intubation, and dacryocystorhinostomy (DCR).
Acquired Nasolacrimal Duct Obstruction
Acquired NLDO is divided into primary (PANDO — idiopathic, inflammatory/fibrotic) and secondary (SALDO — a specific identifiable cause).
Primary PANDO
PANDO is the most common acquired NLDO in adults, predominantly affecting middle-aged to elderly women. Progressive fibrosis and epithelial loss narrow the nasolacrimal canal, likely related to reduced estrogen levels affecting the nasolacrimal mucosa (analogous to osteoporosis). The bony canal dimensions are measurably smaller in affected women.
Neoplastic: lacrimal sac tumors (may present with bloody tears/reflux and a medial canthal mass, classically above the medial canthal tendon), nasal or sinus tumors extending to the duct
Traumatic / iatrogenic: nasal surgery, overly aggressive probing, facial fractures, orbital decompression surgery
Mechanical: dacryoliths (calcified concretions), rhinoliths, mucoceles compressing the duct from outside
Surgical Treatment
The goal of lacrimal surgery is to restore or create a functional tear drainage pathway from the lacrimal sac into the nasal cavity. The approach depends on the site and extent of obstruction, prior surgery, and nasal anatomy.
1. Probing & Irrigation
First-line for congenital NLDO after failed conservative management
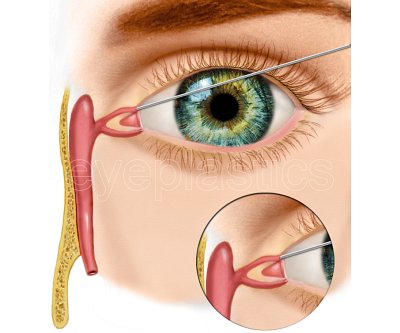
Lacrimal probe passed through punctum into the nasolacrimal duct under topical or general anesthesia
Success rate: ≈ 90% in infants under 12 months; declines with age
Often combined with silicone intubation to prevent re-stenosis
2. Balloon Dacryoplasty
Deflated balloon catheter (LacriCATH®) inserted into the nasolacrimal duct; inflated to approximately 8 atmospheres for 90 seconds at two positions within the duct
Alternative to intubation for refractory congenital NLDO and some adult cases of functional stenosis
Minimal scarring; performed under general anesthesia
3. Endoscopic DCR (Dacryocystorhinostomy)
Endoscopic DCR is a well-established approach for acquired NLDO in adults, chronic dacryocystitis, and failed probing with intubation in children, with success comparable to external DCR. A new bony window is created between the lacrimal sac and the nasal cavity under direct endoscopic visualization, bypassing the blocked nasolacrimal duct entirely.
Step-by-Step Procedure
Anesthesia: General anesthesia (standard) or local anesthesia with IV sedation. Topical vasoconstrictors applied intranasally
Nasal access: Endoscope introduced through the nostril; middle turbinate reflected to expose the lateral nasal wall adjacent to the lacrimal bone
Lacrimal sac identification: Fine probe passed through the punctum transilluminates the sac through the nasal mucosa for precise localization
Bony ostium creation: Nasal mucosa elevated; lacrimal bone and anterior maxilla removed with powered instrumentation (microdebrider and Kerrison rongeur) to create a 10–12 mm bony opening into the lacrimal sac
Mucosal flap: Nasal mucosa fashioned into flaps to line the new anastomosis and promote primary healing
Sac marsupialization: Lacrimal sac opened and apposed to nasal mucosa to create a wide, epithelialized rhinostomy
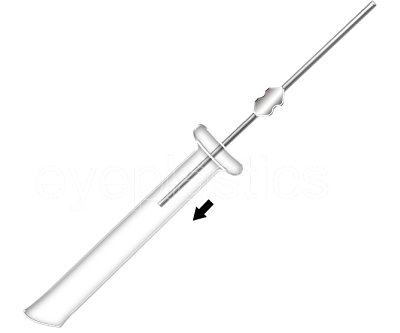
Silicone stent: Bicanalicular silicone tube threaded from each punctum through the rhinostomy and retrieved nasally; removed in clinic at approximately 3 months
Closure: Absorbable nasal packing; no skin incision; no external scar
Recovery
Same-day outpatient procedure; home the same day
Oral antibiotics, antibiotic eye drops, and nasal saline sprays for 2 weeks
Avoid nose blowing for 2 weeks; expect mild bloody nasal discharge for several days
Success rate: 85–95% resolution of tearing
4. External DCR
Incision at the medial canthus; direct access to the lacrimal sac and nasolacrimal duct
Preferred when intranasal anatomy (tumors, severe deviation, prior sinus surgery) prevents an endoscopic approach, or when lacrimal sac biopsy is needed for suspected tumor
Success rate comparable to endoscopic DCR; small external scar hides in the nasofacial groove and is rarely noticeable
Silicone stent placed and removed at 3 months
5. CDCR / Jones Tube
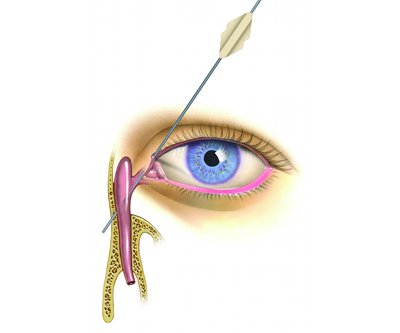
When the canalicular system is too scarred or absent to use (severe canalicular stenosis, canalicular trauma, failed multiple DCRs), a Jones tube (Pyrex glass bypass tube) is implanted to create a direct channel from the inner corner of the eye to the nasal cavity.
The tube bypasses the entire canalicular and sac system
Permanent implant; requires long-term follow-up to monitor tube position and patency
Tubes may require adjustment or replacement over time
Patients must be able to occlude the tube with the finger to blow the nose
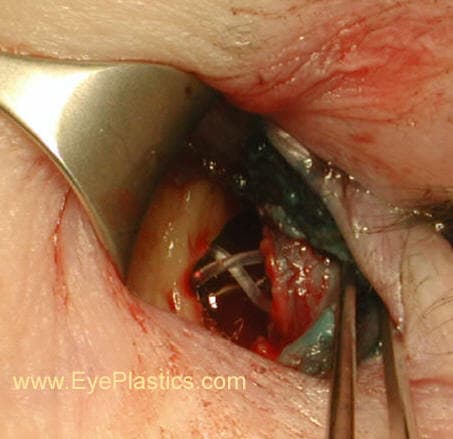
DCR in the Operating Room
Dacryocystorhinostomy creates a new, direct passage from the tear sac into the nose, bypassing the blocked duct. Intraoperative views below show the surgical exposure and the opened lacrimal sac.
Surgical exposure of the lacrimal sacThe opened sac — a new passage into the nose
Frequently Asked Questions
What is a DCR (dacryocystorhinostomy)?
DCR is the surgery that bypasses a blocked tear duct by creating a new drainage opening between the tear sac and the nose, restoring tear drainage. It can be done externally or endonasally.
Will I have a scar from tear-duct surgery?
Endonasal (endoscopic) DCR leaves no skin incision. External DCR uses a small, well-hidden incision beside the nose that typically heals inconspicuously.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in blocked tear duct & dcr surgery.