SOOF Lift (Sub-Orbicularis Oculi Fat Lift)
The sub-orbicularis oculi fat (SOOF) lift resuspends the deep cheek fat pad over the orbital rim — the central maneuver of a midface lift, restoring volume at the tear trough and lid-cheek junction.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
SOOF Lift (Sub-Orbicularis Oculi Fat Lift)
A SOOF lift repositions the sub-orbicularis oculi fat — a deep fat pad that sits beneath the muscle of the lower eyelid, directly over the cheekbone. As we age this pad descends, hollowing the under-eye and flattening the cheek. Lifting and resuspending it restores volume exactly where age-related hollowing shows most: at the lid-cheek junction and the tear trough. It is almost always performed as part of a lower-eyelid or midface procedure rather than on its own.
This is a focused companion to our main Midface / Cheek Lift guide, where the SOOF lift is one of several techniques used to rejuvenate the lid-cheek junction.

What the SOOF Is, and Why It Matters
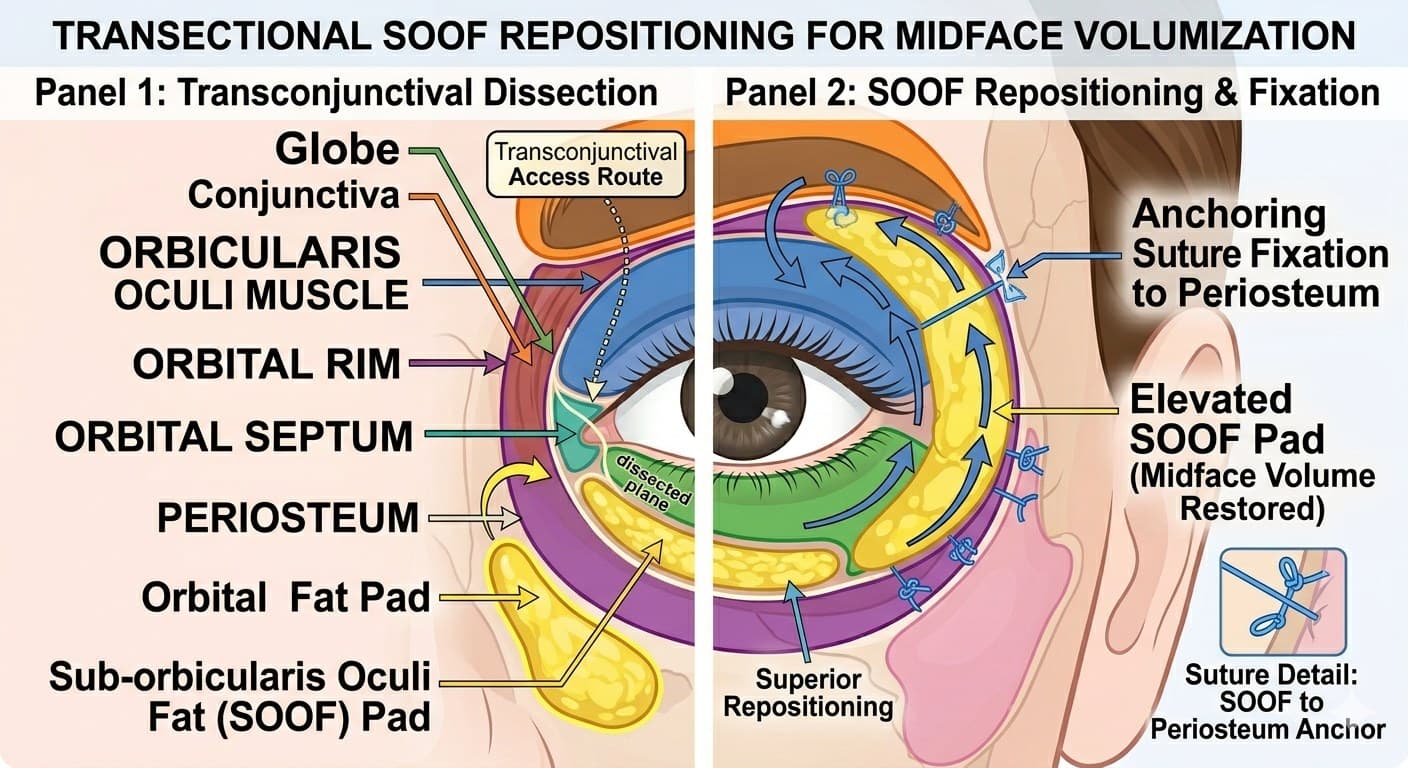
The lower eyelid and cheek are layered, from the surface inward: skin, the orbicularis oculi muscle, then the sub-orbicularis oculi fat (SOOF), and finally the periosteum lining the bone of the inferior orbital rim. The SOOF sits deep to the muscle and superficial to the bone. With age, the retaining ligaments that tether these layers weaken, and the soft tissue — including the SOOF — slides downward and inward in a predictable vector. The tear trough is essentially the visible surface sign of this descent: as the cheek fat falls away from its fixed ligamentous attachment at the rim, a groove appears.
Because the SOOF lies directly over the orbital rim, elevating and re-anchoring it restores projection precisely where the hollow is deepest. That is why SOOF elevation is the central maneuver of most modern midface lifts, and why it pairs so naturally with lower blepharoplasty.
Who Is a Candidate
The SOOF lift addresses descent and hollowing, not fine skin wrinkling. The best candidates show:
- A deep tear trough and a visible step-off at the lid-cheek junction
- A "double-convexity" contour — a lower-lid bulge, a hollow, then the cheek mound below
- A lengthened distance from the lash line to the cheek (a youthful junction is short and seamless)
- Mild lower-lid retraction or scleral show, where SOOF resuspension adds midface support
Patients whose main concern is volume loss alone (rather than true tissue descent) may do better with a filler or fat-grafting approach; those with significant excess skin may need it combined with a skin-tightening procedure. An in-person examination sorts this out.
How the Procedure Works
Access is usually transconjunctival — through the inside of the lower eyelid, leaving no external scar — or through a lower-lid skin crease when a blepharoplasty is done at the same time. The surgeon reaches the SOOF at the level of the inferior orbital rim, mobilizes it off the bone, and elevates it to a higher, more youthful position, fixing it with sutures anchored to the periosteum (the tough lining of the bone) or the deep tissue at the rim. Repositioning the fat, rather than removing it, is what restores contour instead of creating a hollowed, operated look.
The maneuver is frequently combined with lower blepharoplasty (to address a fat bulge or excess skin) and with tear-trough correction, because the same incision reaches all three problems.
Recovery and Results
Expect swelling and bruising for one to two weeks; the deep dissection over the rim means midface swelling can take longer to settle than a simple eyelid procedure. Because the fat is anchored into a new position, the final contour continues to refine over several months as healing completes. Results are durable, since the correction re-suspends the patient's own tissue rather than relying on filler that resorbs.
When to See a Specialist
Because the SOOF sits millimeters from the eye and the correction hinges on precise anchoring at the orbital rim, this is surgery best performed by an oculoplastic surgeon who operates in this plane routinely. An ASOPRS-trained oculoplastic surgeon can determine whether a SOOF lift — alone or with lower blepharoplasty and tear-trough work — is the right approach for your anatomy.
Considering a SOOF lift or midface rejuvenation?
The lid-cheek junction is one of the most delicate areas in facial surgery. Find an ASOPRS-trained oculoplastic surgeon near you.
Frequently Asked Questions
- Is a SOOF lift the same as a lower blepharoplasty?
- No. A lower blepharoplasty addresses eyelid skin and fat bulges; a SOOF lift resuspends the deep cheek fat over the orbital rim. They are frequently done together through the same incision because they solve different parts of the same lid-cheek problem.
- Does a SOOF lift leave a scar?
- Usually not visibly. Access is most often transconjunctival — through the inside of the lower eyelid — leaving no external scar. When combined with a skin-based lower blepharoplasty, the incision sits in a lower-lid crease.
- How long do SOOF lift results last?
- Because the procedure resuspends your own tissue rather than adding filler that resorbs, results are durable, refining over several months as healing completes.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in soof lift (sub-orbicularis oculi fat lift).
Search the Directory →