
Qu'est-ce que la blépharite à Demodex
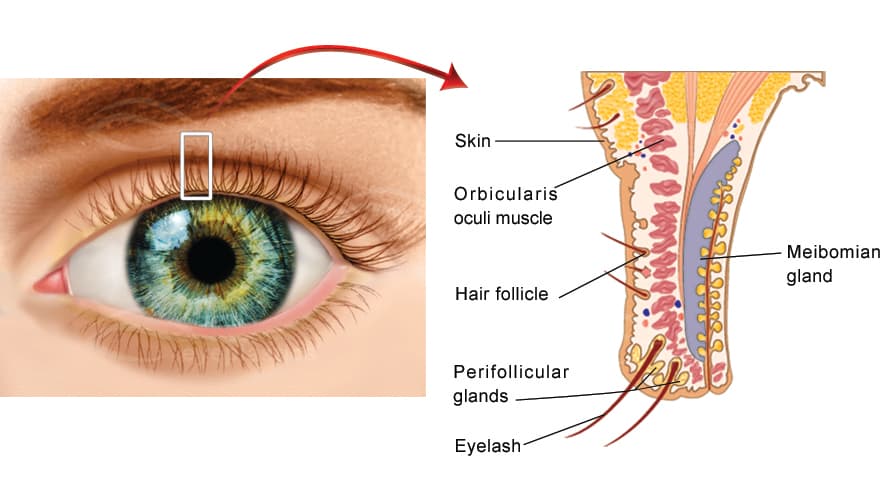
La blépharite à Demodex est une inflammation chronique des marges palpébrales causée par une surpopulation d'acariens microscopiques Demodex qui vivent dans et autour des follicules de cils et des glandes sébacées (glandes de Meibomius) des paupières. C'est l'une des causes les plus fréquentes — et les plus souvent méconnues — de blépharite. Les acariens sont un habitant normal de la peau humaine, mais lorsque leur nombre augmente, ils déclenchent une irritation du bord de la paupière, les débris cireux caractéristiques appelés collerettes, et un cycle de démangeaisons, de rougeur et d'instabilité du film lacrymal.
Cette page est le complément détaillé de notre guide principal sur la Blépharite. Demodex chevauche largement la dysfonction de la glande de Meibomius (DGM), la sécheresse oculaire, et la rosacée oculaire — ces conditions sont souvent traitées ensemble.
Les deux acariens à l'origine de la maladie
Deux espèces apparentées causent la maladie de Demodex oculaire, et elles ont tendance à produire deux modèles différents de blépharite :
Demodex folliculorum
Vit à l'intérieur du follicule de cil, généralement en grappes autour de la racine du cil.
- Provoque une blépharite antérieure
- Produit les collerettes cylindriques enroulées autour de la base du cil
- Associée à la malposition des cils, à la chute des cils et à une irritation récurrente
Demodex brevis
S'enfonce plus profondément dans les glandes de Meibomius et les glandes sébacées.
- Contribue à la blépharite postérieure et à la DGM
- Obstrue les orifices glandulaires, aggravant la sécheresse évaporative
- Liée aux chalazions récurrents
Parce que les deux espèces occupent différentes parties de la paupière, nombreux patients présentent un tableau mixte — collerettes antérieures et obstruction de la glande de Meibomius — ce qui explique pourquoi Demodex est si souvent intriqué à la sécheresse oculaire et à la DGM.
Collerettes — Le signe révélateur
Les collerettes — parfois appelées pellicules cylindriques — sont des manchons cireux et translucides de déchets d'acariens et de débris cutanés qui forment une gaine claire autour de la base des cils. Elles sont considérées comme pathognomoniques pour Demodex : si un patient a des collerettes, il a une blépharite à Demodex. Contrairement aux écailles dures et cassantes (squames) de la blépharite staphylococcique, les collerettes sont molles, semi-transparentes et glissent le long du cil au fur et à mesure qu'il pousse.
Conseil clinique : Les collerettes sont mieux visibles en demandant au patient de regarder vers le bas tout en examinant les cils de la paupière supérieure à la lampe à fente. Leur présence et leur nombre sont maintenant utilisées pour évaluer la gravité de la maladie et pour suivre la réponse au traitement.
Qui l'attrape
La colonisation par Demodex augmente régulièrement avec l'âge — elle est pratiquement universelle chez les personnes âgées — mais la maladie symptomatique peut survenir à tout âge. Les associations reconnues incluent :
- L'âge avancé — le facteur de risque unique le plus important
- La rosacée faciale et oculaire — fortement liée à la surpopulation de Demodex
- La blépharite chronique, la DGM et la sécheresse oculaire qui n'ont pas répondu à l'hygiène palpébrale standard
- Les chalazions ou orgeolets récurrents
- La peau grasse (séborrhée), le diabète et l'immunodépression
- Le port prolongé de lentilles de contact et le retrait incomplet du maquillage oculaire
Symptômes
- Démangeaisons des marges palpébrales — souvent la plainte dominante, classiquement pire le matin
- Sensation de brûlure, de corps étranger ou de grattement
- Marges palpébrales rouges, irritées, croûteuses avec des débris à la base des cils
- Yeux larmoyants alternant avec sécheresse et vision floue fluctuante dépendante du clignement
- Cils qui semblent collants, cassants, mal dirigés, ou qui tombent (madarose)
- Chalazions récurrents et sensation que « rien de ce que le patient essaie ne marche complètement »
Diagnostic
La blépharite à Demodex est diagnostiquée à la lampe à fente — aucun test sanguin ou culture n'est requis :
- Identification des collerettes : La découverte de collerettes cylindriques à la base des cils confirme le diagnostic. Le nombre de cils présentant des collerettes est utilisé pour évaluer la gravité.
- Rotation du cil / microscopie après épilation : Faire tourner ou épiler un cil et l'observer au microscope révèle directement les acariens — le test de confirmation historique.
- Évaluation de la marge palpébrale et de Meibomius : L'évaluation des orifices de Meibomius obstrués, des télangiectasies et du temps de rupture du film lacrymal réduit identifie la DGM et la sécheresse oculaire coexistantes.
Traitement
Les objectifs du traitement sont de réduire la population d'acariens, d'éliminer les collerettes, de calmer l'inflammation et de gérer la sécheresse oculaire et la dysfonction des glandes de Meibomius qui l'accompagnent généralement. Comme les acariens se reproduisent, la blépharite à Demodex est gérée comme une condition chronique et récidivante plutôt que comme une cure ponctuelle.
Traitement sur ordonnance — lotilaner (XDEMVY™)
XDEMVY (solution ophtalmologique de lotilaner 0,25 %) est le premier et le seul traitement sur ordonnance approuvé par la FDA spécifiquement pour la blépharite à Demodex. Le lotilaner paralyse et tue les acariens en ciblant leur système nerveux. Il est administré sous forme d'une goutte dans chaque œil deux fois par jour pendant six semaines. Dans les essais de phase 3 Saturn-1 et Saturn-2, une proportion significativement plus importante de patients traités ont atteint une cure de collerette (réduction à pas plus de deux collerettes) et une éradication des acariens par rapport au véhicule — environ la moitié des patients traités ont atteint la cure de collerette — l'effet secondaire le plus courant étant une légère sensation de piqûre ou de brûlure transitoire à l'instillation.
Hygiène des paupières et huile d'arbre à thé
- Terpinen-4-ol (dérivé de l'huile d'arbre à thé) : Le principe actif de l'huile d'arbre à thé ayant une activité anti-Demodex. Disponible sous forme de lingettes et de nettoyants pré-humidifiés (p. ex., OCuSOFT Lid Scrub Oust Eyelid Cleanser, Cliradex) pour un usage quotidien à domicile. L'huile d'arbre à thé concentrée est irritante et ne doit pas être appliquée non diluée près de l'œil.
- Le spray d'acide hypochloreux et les nettoyants commerciaux des paupières réduisent la charge bactérienne et du biofilm qui accompagne la surpopulation d'acariens et soutiennent le régime thérapeutique sur ordonnance.
- Les compresses chaudes et le massage des paupières (p. ex., le OCuSOFT Dry Eye Mask) abordent l'obstruction coexistante des glandes de Meibomius.
Procédures au cabinet
- Microblepharoexfoliation (BlephEx) : Débridement mécanique du bord de la paupière avec une micro-éponge rotative pour éliminer les collerettes, le biofilm et les débris.
- Intense Pulsed Light (IPL) : La lumière pulsée périoculaire réduit les populations de Demodex et les télangiectasies associées à la rosacée tout en améliorant la fonction des glandes de Meibomius ; généralement une série de 3 à 4 séances.
- Expression de la glande de Meibomius / pulsation thermique (LipiFlow) : Élimine l'obstruction de la glande provoquée par Demodex brevis.
Traiter toute la paupière. Comme Demodex, la dysfonction des glandes de Meibomius, la sécheresse oculaire et la rosacée se renforcent mutuellement, les résultats les plus durables proviennent de la combinaison d'une thérapie dirigée contre les acariens avec des soins continus des glandes de Meibomius et de la surface oculaire.
Conditions connexes
- Blépharite — la catégorie plus large ; Demodex est l'une de ses causes principales.
- Dysfonction des glandes de Meibomius (DGM) — coexiste fréquemment, provoquée par Demodex brevis.
- Sécheresse oculaire — à la fois une conséquence et un aggravant de Demodex.
- Rosacée oculaire — fortement associée à la surpopulation d'acariens.
- Chalazion — les chalazia récurrents peuvent signaler un Demodex/DGM sous-jacent.
Quand consulter un spécialiste
Consultez un médecin ophtalmologiste ou un spécialiste en chirurgie oculoplastique si vous avez des démangeaisons persistantes des paupières, une rougeur ou une croûte qui ne s'améliore pas avec l'hygiène des paupières en vente libre, des orgelets ou des chalazia récurrents, ou des symptômes de sécheresse oculaire chronique qui n'ont pas réagi aux gouttes. Un simple examen à la lampe à fente pour détecter les collerettes peut confirmer la blépharite à Demodex et ouvrir la porte à un traitement ciblé et efficace.