Eyelash-mite infestation (Demodex folliculorum & brevis) — the cause of collarettes, chronic lid irritation, and a common driver of blepharitis, MGD, and dry eye.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
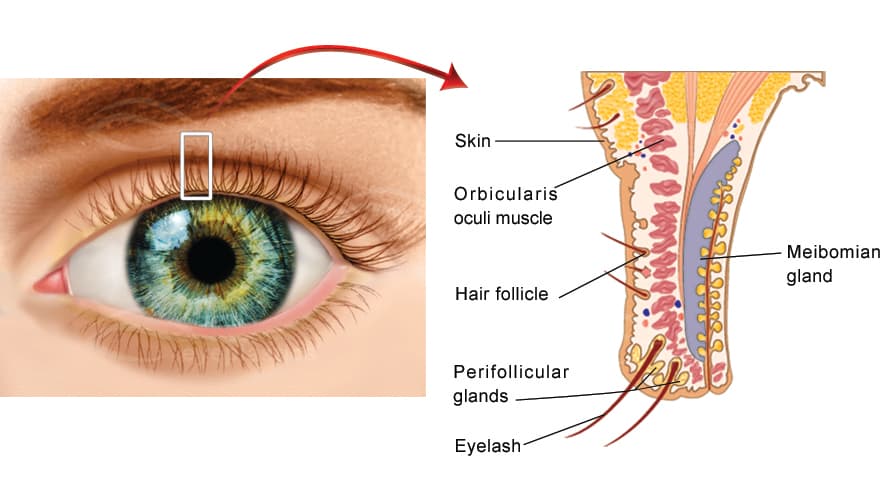
Demodex blepharitis is a chronic inflammation of the eyelid margins caused by an overpopulation of microscopic Demodex mites that live in and around the eyelash follicles and the oil (meibomian) glands of the lids. It is one of the most common — and most frequently missed — causes of blepharitis. Mites are a normal resident of human skin, but when their numbers rise they trigger lid-margin irritation, the characteristic waxy debris called collarettes, and a cycle of itching, redness, and tear-film instability.
This page is the in-depth companion to our main Blepharitis guide. Demodex overlaps heavily with meibomian gland dysfunction (MGD), dry eye disease, and ocular rosacea — the conditions are often treated together.
Two related species cause ocular Demodex disease, and they tend to produce two different patterns of blepharitis:
Demodex folliculorum
Lives inside the eyelash follicle, usually in clusters around the lash root.
Because the two species occupy different parts of the lid, many patients have a mixed picture — anterior collarettes and meibomian gland obstruction — which is why Demodex is so often intertwined with dry eye and MGD.
Collarettes — sometimes called cylindrical dandruff — are translucent, waxy cuffs of mite waste and skin debris that form a clear sleeve around the base of the eyelashes. They are considered pathognomonic for Demodex: if a patient has collarettes, they have Demodex blepharitis. Unlike the hard, brittle scales (scurf) of staphylococcal blepharitis, collarettes are soft, semi-clear, and slide up the lash as it grows.
Clinical pearl: Collarettes are best seen by asking the patient to look down while examining the upper lid lashes at the slit lamp. Their presence and number are now used to grade disease severity and to track response to treatment.
Demodex colonization rises steadily with age — it is nearly universal in the elderly — but symptomatic disease can occur at any age. Recognized associations include:
Demodex blepharitis is diagnosed at the slit lamp — no blood test or culture is required:
The goals of treatment are to reduce the mite population, clear collarettes, calm inflammation, and manage the dry eye and MGD that usually accompany it. Because mites repopulate, Demodex blepharitis is managed as a chronic, relapsing condition rather than a one-time cure.
XDEMVY (lotilaner ophthalmic solution 0.25%) is the first and only FDA-approved prescription treatment specifically for Demodex blepharitis. Lotilaner paralyzes and kills the mites by targeting their nervous system. It is dosed as one drop in each eye twice daily for six weeks. In the phase 3 Saturn-1 and Saturn-2 trials, a significantly greater proportion of treated patients achieved collarette cure (reduction to no more than two collarettes) and mite eradication compared with vehicle — roughly half of treated patients reached collarette cure — with the most common side effect being mild, transient stinging or burning at instillation.
Treat the whole lid. Because Demodex, MGD, dry eye, and rosacea reinforce one another, the most durable results come from combining mite-directed therapy with ongoing meibomian gland and ocular-surface care.
See an eye physician or oculoplastic specialist if you have persistent eyelid itching, redness, or crusting that does not improve with over-the-counter lid hygiene, recurrent styes or chalazia, or chronic dry-eye symptoms that have not responded to drops. A simple slit-lamp examination for collarettes can confirm Demodex blepharitis and open the door to targeted, effective treatment.
Connect with a board-certified oculoplastic surgeon who specializes in demodex blepharitis.
Search the Directory →