Balloon Dacryoplasty
Balloon dacryoplasty is a minimally invasive way to open a narrowed or blocked tear-drainage duct without creating an external incision. A tiny deflated balloon catheter is threaded into the nasolacrimal duct and inflated to stretch open the narrowed segment — much like an angioplasty balloon opens a narrowed blood vessel. It is used chiefly for stubborn congenital tear-duct obstruction in children and for some adults with a partial (functional) narrowing.
This is a focused companion to our main Tearing & the Lacrimal System guide and our detailed Blocked Tear Duct & DCR page, which cover the full range of tear-duct procedures.
How Balloon Dacryoplasty Works
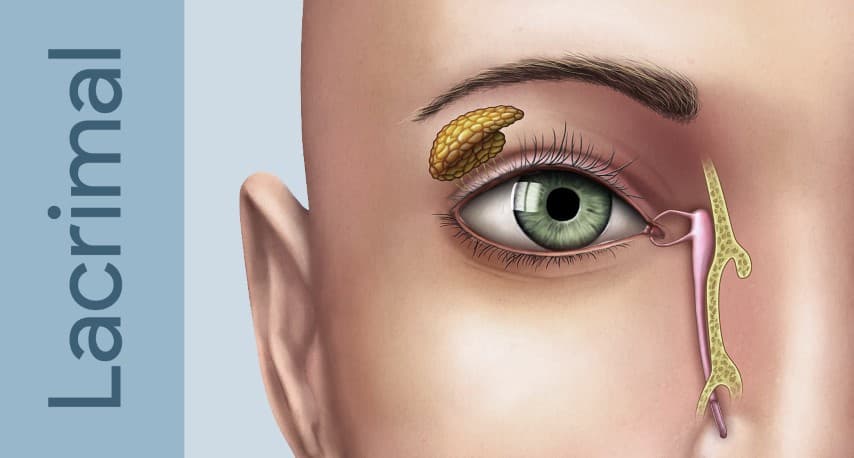
The tear-drainage system carries tears from the eye's surface, through the puncta (the tiny openings at the inner corner of the lids), down the nasolacrimal duct into the nose. When that duct is narrowed rather than completely scarred shut, a balloon can reopen it:
- A deflated balloon catheter (such as the LacriCATH®) is passed through the punctum into the nasolacrimal duct
- It is inflated to roughly 8 atmospheres of pressure for about 90 seconds, at two positions along the duct, to dilate the narrowed segment
- The balloon is deflated and withdrawn, leaving no incision and minimal scarring
The procedure is performed under general anesthesia, most often in children. It can be used on its own or combined with silicone intubation (a soft temporary stent) to keep the duct open while it heals.
Who Is a Candidate
Balloon dacryoplasty is best suited to:
- Children with congenital nasolacrimal duct obstruction that has not resolved after simple probing, especially older infants and toddlers where a plain probe alone is less reliable
- Adults with a partial or "functional" stenosis — a duct that is narrowed and sluggish rather than fully blocked
It is an alternative to intubation for refractory congenital cases. When the duct is completely scarred shut, or blocked by chronic infection of the tear sac (dacryocystitis), a balloon cannot reopen it — those cases need a bypass operation (dacryocystorhinostomy, or DCR), which creates a new drainage pathway directly into the nose.
Where It Fits Among Tear-Duct Procedures
Think of tear-duct treatment as a ladder, from least to most invasive:
- Probing — a fine probe opens a congenital blockage; success is about 90% in infants under 12 months and declines with age
- Silicone intubation — a soft stent holds the duct open during healing, often after probing
- Balloon dacryoplasty — stretches open a narrowed segment, for refractory or older cases
- DCR — the definitive bypass when the duct is truly blocked
Choosing the right rung depends on the child's age, whether prior probing failed, and whether the obstruction is a narrowing or a complete block.
Recovery
Because there is no incision, recovery is quick. Children typically go home the same day. Antibiotic-steroid drops are used for a short period, and if a stent was placed it is removed in the office weeks to months later. Tearing usually improves as the duct heals and any swelling settles.
When to See a Specialist
Persistent tearing, discharge, or recurrent tear-sac infections deserve evaluation — particularly in a child whose watering has not resolved by their first birthday, or an adult with a chronically wet, irritated eye. An ASOPRS-trained oculoplastic surgeon can determine whether a balloon dacryoplasty, intubation, or a DCR is the right next step.
A watery or infected tear duct has a solution
From minimally invasive balloon dacryoplasty to definitive DCR surgery, an oculoplastic surgeon can open the drainage the right way. Find a specialist near you.