Lacrimal System
Treatment of blocked tear ducts, chronic tearing, dacryocystorhinostomy (DCR), and lacrimal infections — adult and pediatric.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
The Lacrimal System
The lacrimal system is the eye’s tear apparatus — the glands that produce tears and the channels that drain them away. With every blink, a thin tear film is spread across the surface of the eye, keeping it lubricated, optically clear, and protected against infection; the used tears then drain through tiny openings at the inner corner of the eyelids, down through the tear sac and nasolacrimal duct, and into the nose. Because this single system both makes and removes tears, the problems that arise fall into two broad groups: insufficient tears or an unstable tear film, which leaves the eye dry, gritty, and irritated, and impaired drainage, which causes a constantly watering eye (epiphora), mucous discharge, and recurrent infection of the tear sac (dacryocystitis). The sections below follow the tears along this pathway — from how they drain, through the relevant anatomy, to the evaluation and surgical treatment of blockage.
The lacrimal system produces, distributes, and drains tears. A healthy tear film is essential for corneal health, clear vision, and comfort. When any part of the drainage pathway is blocked, tears overflow onto the cheek (epiphora), stagnate in the drainage sac, and become a reservoir for infection.
How Tears Drain
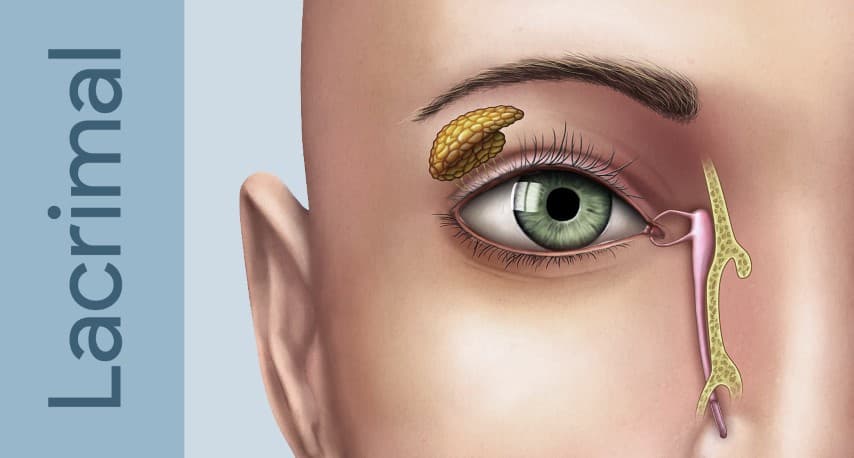
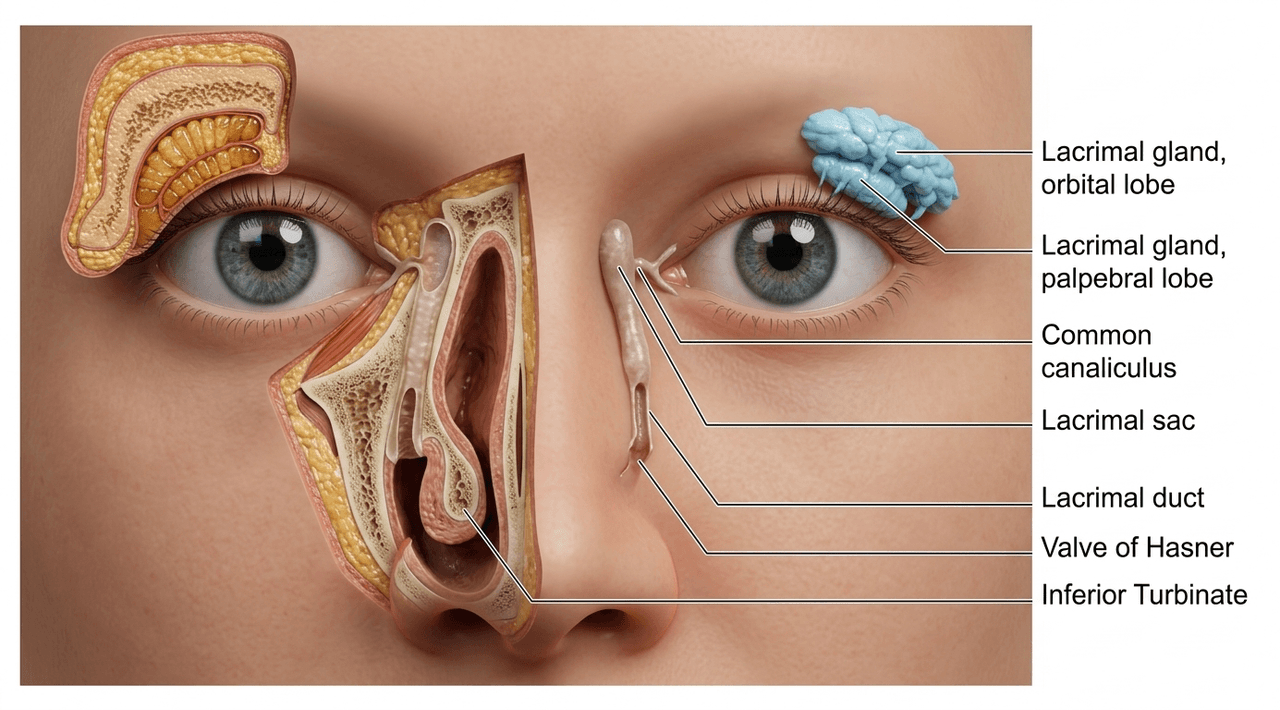
- The lacrimal gland (upper outer orbit) and accessory glands produce the aqueous tear layer
- Blinking sweeps tears medially toward the inner corner of the eye
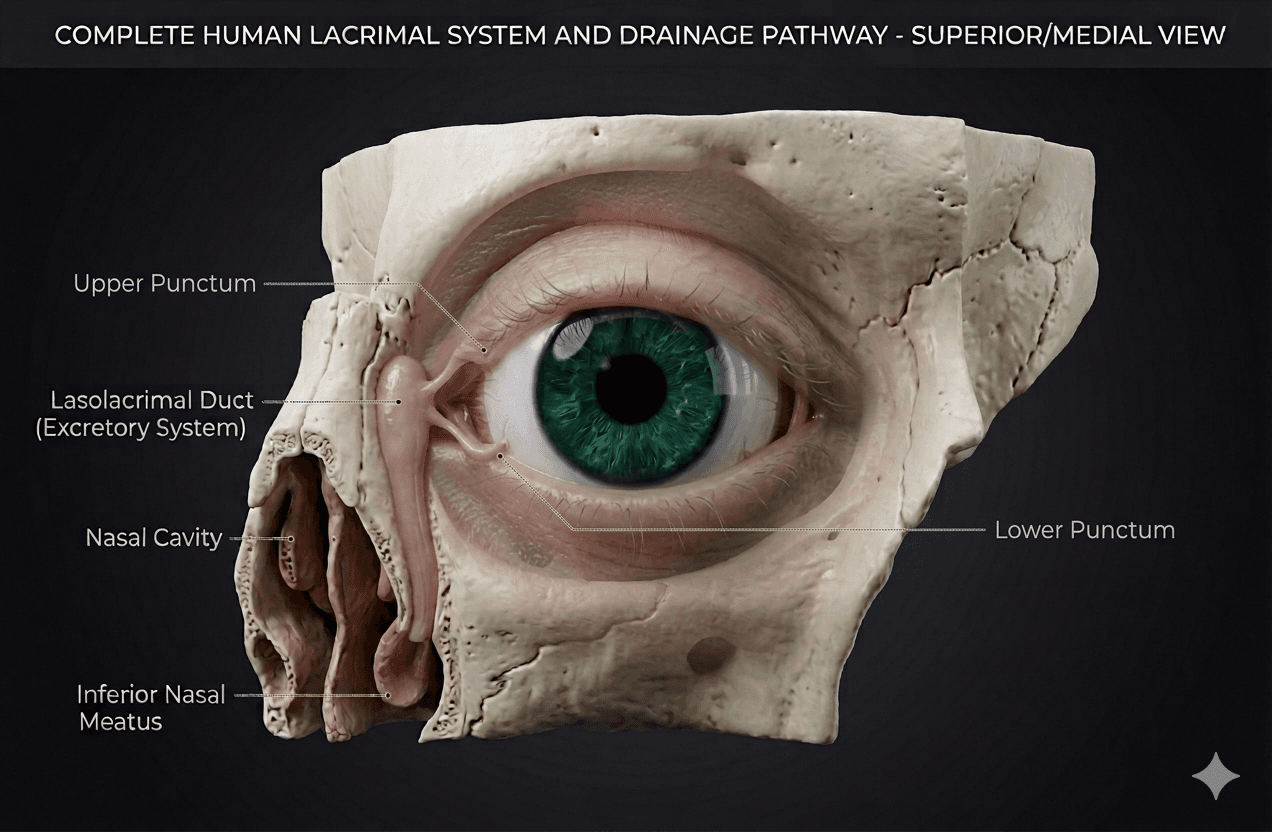
- Tears enter the puncta (small openings at the inner corner of each eyelid), travel through the canaliculi, and collect in the lacrimal sac
- From the sac, tears drain through the nasolacrimal duct and exit under the inferior turbinate in the nose (valve of Hasner)
Symptoms of Obstruction
- Excessive tearing (tears spilling over the eyelid margin — epiphora)
- Mucous or purulent discharge, especially in the morning
- Recurrent red eye or conjunctivitis
- Painful, swollen inner corner of the eyelid (acute dacryocystitis)
- Secondary skin changes or maceration of the lower lid skin
For a detailed overview of lacrimal anatomy, see the Anatomy Overview or the dedicated Lacrimal Anatomy page.
Lacrimal Anatomy
Understanding the anatomy guides both the diagnostic work-up and the choice of surgical repair. The drainage system has several potential sites of obstruction:
- Punctal stenosis: the opening is too small or closed; common in elderly patients and after topical medication use
- Canalicular obstruction: the canaliculi (upper and lower) may be scarred by infection, trauma, or chemotherapy agents (especially 5-FU and docetaxel)
- Common canalicular obstruction: where the upper and lower canaliculi join before entering the lacrimal sac
- Nasolacrimal duct obstruction (NLDO): the most common site; the duct narrows or occludes at or just above the valve of Hasner
Explore the Lacrimal System
Tear-drainage problems range from a simply watery eye to blocked ducts, infections, and injuries. Explore each in depth:
Frequently Asked Questions
- What causes a blocked tear duct?
- The most common cause in adults is involutional stenosis — gradual narrowing of the nasolacrimal duct with age. Other causes include infection (dacryocystitis), trauma, nasal or sinus surgery, certain eye drops (glaucoma medications), and inflammatory diseases. In infants, blocked tear ducts are usually due to a membrane at the lower end of the duct that fails to open at birth.
- What is DCR surgery?
- Dacryocystorhinostomy (DCR) is the surgical bypass of a blocked nasolacrimal duct. A new drainage opening is created directly between the lacrimal sac and the nasal cavity, bypassing the blocked duct entirely. DCR can be performed externally (through a small incision beside the nose) or endoscopically (through the nose, with no external incision).
- What is the success rate of DCR surgery?
- External DCR has long-term success rates of approximately 90–95%. Endoscopic DCR has similar success rates in experienced hands. Most patients experience complete relief of tearing after surgery.
- Can a child's blocked tear duct resolve without surgery?
- Yes — up to 90% of congenital nasolacrimal duct obstructions in infants resolve spontaneously by 12 months with massage and topical antibiotics for infections. If the obstruction persists at 12–18 months, a simple probing procedure is performed under brief anesthesia.
- What should I expect during my lacrimal system consultation?
- During your consultation, your oculoplastic surgeon will review your symptoms, examine your eyes and tear drainage system, and may perform diagnostic tests such as dye tracing or imaging to identify the exact location and cause of the blockage. They will discuss your treatment options, explain the recommended procedure, and answer any questions about what to expect before and after treatment. This appointment helps ensure you're a good candidate for surgery and allows you to make an informed decision about your care.
- What is the recovery timeline after lacrimal surgery?
- Most patients experience some mild discomfort, swelling, and drainage for the first 1-2 weeks following lacrimal surgery. You can typically return to light activities within a few days, though strenuous exercise and heavy lifting should be avoided for 2-3 weeks to prevent complications. Complete healing of the surgical site takes several weeks, and your surgeon will provide specific instructions on eye drops, nasal saline rinses, and activity restrictions to support proper healing.
- Are there risks or complications associated with lacrimal surgery?
- Like any surgical procedure, lacrimal surgery carries some risks, including infection, bleeding, and temporary or persistent tearing. In rare cases, the surgical site may scar and narrow over time, requiring revision surgery. Your surgeon will discuss all potential complications during your consultation and explain how they minimize these risks through advanced surgical techniques and proper post-operative care instructions.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in lacrimal system.
Search the Directory →