Eyelid Anatomy
The eyelid is a remarkably complex structure — five distinct tissue layers work together to protect the eye, distribute the tear film, and regulate the amount of light entering. Understanding this anatomy is the foundation for all oculoplastic procedures.
Overview
Each eye is protected by upper and lower eyelids (palpebrae). The eyelids meet at two corners — the medial canthus (near the nose) and the lateral canthus (toward the temple). The free margin of each lid is approximately 30 mm long and carries two to three rows of lashes (cilia).
The upper eyelid normally rests 1–2 mm below the superior limbus of the cornea. The lower lid rests at or just above the inferior limbus. Any deviation from these positions — whether drooping, turning in, or turning out — is a surgical indication that oculoplastic surgeons are trained to correct.
Eyelid Layers
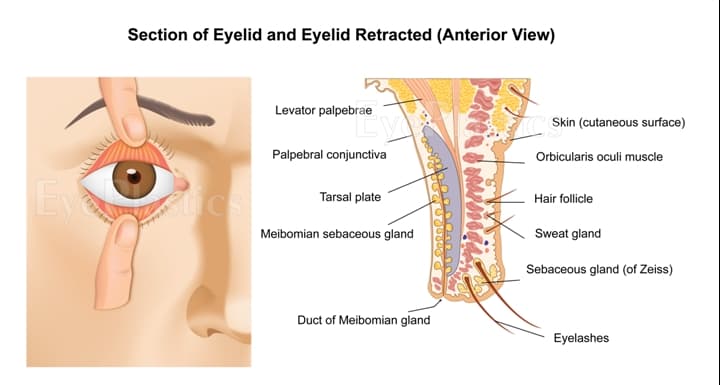
From anterior (front) to posterior (back), the eyelid consists of five layers:
- 1Skin
The thinnest skin in the body — typically 0.5–1 mm. It contains fine hair follicles and sebaceous glands, and becomes redundant with age, contributing to dermatochalasis (hooded lids).
- 2Orbicularis Oculi
A circular muscle responsible for eyelid closure. The orbital portion closes forcefully (blink, squint); the preseptal and pretarsal portions perform gentle, reflex blinking. Paralysis of this muscle — as in facial nerve palsy — causes lagophthalmos (inability to close the eye).
- 3Orbital Septum
A fibrous membrane that acts as the anterior boundary of the orbit, keeping orbital fat behind the eyelid. The septum fuses with the levator aponeurosis in the upper lid and the capsulopalpebral fascia in the lower lid. Septal weakness allows prolapse of orbital fat ("bags under the eyes").
- 4Tarsus (Tarsal Plate)
A dense fibrous plate that provides structural rigidity to the eyelid. The upper tarsus is roughly 10–12 mm in height; the lower tarsus 3–4 mm. It contains the Meibomian glands, which secrete the lipid layer of the tear film. The tarsus is the key landmark in most eyelid reconstructive procedures.
- 5Conjunctiva
A transparent mucous membrane lining the posterior surface of the lid and folding forward to cover the anterior sclera. It contains goblet cells that contribute to the mucin layer of the tear film. The palpebral conjunctiva is firmly adherent to the tarsus; the bulbar conjunctiva covers the globe.
Upper Eyelid Anatomy
The upper eyelid is primarily opened (elevated) by two muscles:
Levator Palpebrae Superioris
The primary elevator of the upper lid. It originates from the lesser wing of the sphenoid bone at the orbital apex, travels anteriorly above the superior rectus muscle, and fans out into a broad aponeurosis that inserts into the anterior surface of the tarsal plate and skin (creating the lid crease). The levator is innervated by the oculomotor nerve (CN III). Dysfunction — from neurological, muscular, or aponeurotic causes — produces ptosis.
Müller's Muscle
A smooth muscle that provides 1–3 mm of additional lid elevation. It originates from the undersurface of the levator and inserts onto the superior tarsal border. It is under sympathetic innervation — which is why Horner's syndrome (disrupted sympathetics) causes a partial 2 mm ptosis. Phenylephrine drops, which stimulate sympathetic receptors, are used diagnostically to predict response to Müller's muscle resection surgery.
Superior Orbital Fat Compartments
The upper lid contains two fat compartments: the central (preaponeurotic) fat and the medial fat pad (which is paler and more fibrous). These lie behind the orbital septum, anterior to the levator. Prolapse or herniation of this fat forward creates upper lid fullness. The lacrimal gland occupies the superolateral orbit and should not be mistaken for fat during blepharoplasty.
Lower Eyelid Anatomy
The lower eyelid lacks a true retractor muscle comparable to the levator. Inferior retraction is provided by the capsulopalpebral fascia — an extension of the inferior rectus muscle sheath that inserts onto the inferior tarsal border. Below the tarsus, the orbital septum contains three fat compartments:
- Medial fat pad — separated from the central compartment by the inferior oblique muscle
- Central fat pad — the most prominent; herniation creates the classic infraorbital "bag"
- Lateral fat pad — smaller, less commonly symptomatic
The lower lid position is primarily maintained by the canthal tendons and orbicularis tone. When these weaken with age, the lid may turn inward (entropion) or outward (ectropion) — two of the most common oculoplastic conditions.
Canthal Tendons
Medial Canthal Tendon
A fibrous band anchoring the medial ends of both tarsal plates to the anterior and posterior lacrimal crests of the maxillary bone. It has an anterior limb (the dominant attachment) and a posterior limb. The posterior limb passes behind the lacrimal sac and helps propel tears into the nasolacrimal duct through the "lacrimal pump" mechanism. Laxity of this tendon causes medial ectropion and epiphora.
Lateral Canthal Tendon
Anchors the lateral tarsal ends to the orbital tubercle of the zygomatic bone, approximately 2 mm inside the orbital rim. Laxity of the lateral canthal tendon is the most common cause of involutional ectropion. Lateral canthopexy or canthoplasty — procedures that tighten or reattach this tendon — are the cornerstone of lower eyelid laxity repair.
Lacrimal Drainage
Tears are produced by the lacrimal gland (superolateral orbit) and accessory lacrimal glands (conjunctiva). They flow across the ocular surface and drain medially through the lacrimal drainage system:
- Puncta — two small openings on the medial upper and lower lid margins
- Canaliculi — small canals leading medially, joining into a common canaliculus
- Lacrimal sac — a small reservoir in the medial canthal area
- Nasolacrimal duct — drains inferiorly into the inferior nasal meatus
Obstruction anywhere along this pathway causes epiphora (tearing). The eyelid's "lacrimal pump" — powered by the orbicularis and medial canthal tendon — actively propels tears through the system with each blink.
Fitzpatrick Skin Phototypes
The Fitzpatrick classification divides skin into six phototypes based on response to ultraviolet exposure. For eyelid surgery and skin tumor management, phototype influences healing characteristics, hyperpigmentation risk, keloid tendency, and skin cancer incidence.
| Type | Skin Color | Sun Response | Typical Features |
|---|---|---|---|
| I | Very fair / ivory | Always burns, never tans | Red or blonde hair; blue/green eyes; freckles |
| II | Fair / pale | Usually burns, rarely tans | Light hair; blue, hazel, or green eyes |
| III | Medium / beige | Sometimes burns, gradually tans | Any hair color; green, hazel, or light brown eyes |
| IV | Olive / light brown | Rarely burns, tans easily | Dark brown hair and eyes; Mediterranean ancestry |
| V | Brown | Very rarely burns, tans deeply | Dark hair and eyes; Middle Eastern, Hispanic, South Asian |
| VI | Dark brown / black | Never burns, deeply pigmented | Black hair and eyes; Sub-Saharan African ancestry |
Types I–III have the highest risk of UV-induced skin cancer (basal cell carcinoma, squamous cell carcinoma, melanoma). Types IV–VI have lower skin cancer rates but are more prone to post-inflammatory hyperpigmentation and keloid formation following eyelid surgery.
Clinical Relevance
A precise understanding of eyelid anatomy allows Dr. Brown to identify the exact anatomical layer responsible for each patient's condition and to plan surgery that corrects it with the least disruption to surrounding structures.
Dermatochalasis
Excess skin (layer 1)
Upper blepharoplasty →
Orbital fat prolapse
Septal weakness (layer 3)
Fat repositioning or removal →
Ptosis
Levator aponeurosis
Levator repair / Müller's resection →
Ectropion
Canthal tendon laxity
Canthoplasty / canthopexy →
Entropion
Lower lid retractor laxity
Retractor reinsertion + tightening →
Lagophthalmos
Orbicularis weakness
Gold weight implant / tarsorrhaphy →
Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.