Orbital Anatomy
The orbit is a bony pyramid roughly 40 mm deep that houses and protects the eyeball, its six muscles, the optic nerve, and the lacrimal gland. Understanding orbital anatomy is essential for evaluating proptosis, orbital fractures, tumors, and the changes that occur in thyroid eye disease.
Overview
The orbit is shaped like a pear or four-sided pyramid with its apex pointing posteriorly toward the optic canal. It is widest approximately 1 cm behind the orbital rim. Volume is approximately 30 mL in adults, of which the globe occupies about 6.5 mL.
The four walls of the orbit — roof, floor, medial wall, and lateral wall — are each composed of different bones and have different clinical vulnerabilities. The medial wall and floor are the thinnest and most commonly fractured; the lateral wall is the thickest and most surgically accessible.
Orbital Bones
Seven bones contribute to the orbital walls. Click any bone in the interactive diagram below to identify it and learn its anatomical role.

Click any region to identify the orbital bones and foramina.
Frontal bone
Forms the orbital roof and supraorbital rim
Zygomatic bone
Forms the lateral wall and lateral orbital rim — the thickest, most accessible wall
Maxillary bone
Forms the orbital floor and inferior rim; fractures here cause blow-out injuries
Sphenoid bone
Greater and lesser wings form the posterior lateral wall and orbital apex
Ethmoid bone
Forms the medial wall (lamina papyracea — paper-thin); borders the sinuses
Lacrimal bone
Small bone at the medial wall containing the lacrimal sac fossa
Palatine bone
Small contribution to the postero-medial floor near the apex


Extraocular Muscles
Six extraocular muscles (EOMs) control all eye movements. Five arise from the common tendinous ring (annulus of Zinn) at the orbital apex; the inferior oblique originates from the antero-medial orbital floor. Click any muscle in the interactive diagram to identify it.
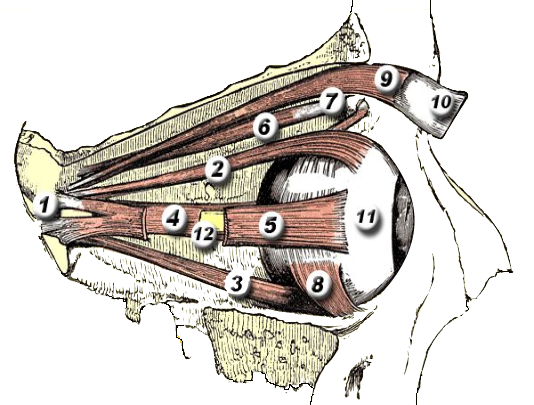
Click any marker to identify the extraocular muscles.
Medial rectus (MR)
Adduction (moves eye inward)
Nerve: CN III
Lateral rectus (LR)
Abduction (moves eye outward)
Nerve: CN VI
Superior rectus (SR)
Elevation, intorsion, adduction
Nerve: CN III
Inferior rectus (IR)
Depression, extorsion, adduction
Nerve: CN III
Superior oblique (SO)
Intorsion, depression, abduction
Nerve: CN IV
Inferior oblique (IO)
Extorsion, elevation, abduction
Nerve: CN III
In thyroid eye disease, inflammation and fibrosis of the extraocular muscles — most commonly the inferior rectus — is a major cause of proptosis, diplopia, and optic nerve compression. Orbital decompression surgery enlarges the bony orbit to provide more space for the swollen muscles and fat.
Orbital Fat Compartments
Orbital fat cushions and supports the globe and optic nerve. It is divided into two main compartments by the extraocular muscles and their intermuscular septa:
- Intraconal fat — inside the muscular cone formed by the four rectus muscles. Contains the optic nerve, ophthalmic artery, and cranial nerves. The most critical surgical space; manipulation here risks optic nerve injury.
- Extraconal fat — outside the muscular cone, between the muscles and the orbital walls. More accessible surgically; the lacrimal gland sits in the superolateral extraconal space.
Increased orbital fat volume — whether from thyroid-related glycosaminoglycan deposition or tumor growth — pushes the globe forward, producing proptosis (exophthalmos). Orbital decompression removes fat and/or bone to reduce this pressure.
Optic Nerve & Orbital Apex
The orbital apex contains the optic canal — through which the optic nerve (CN II) and ophthalmic artery pass — and the superior orbital fissure, which transmits CN III, IV, V1, VI, and the ophthalmic veins.
Optic Canal
Approximately 8–10 mm long, 5 mm wide. The optic nerve has a 20–30 mm course within the orbit — slightly longer than the 18 mm direct distance — giving it a sinuous path that accommodates globe movement without traction.
Optic Nerve Compression
When enlarged extraocular muscles (as in severe thyroid eye disease) compress the optic nerve at the apex, vision loss may occur with normal-appearing visual acuity at first — making color desaturation an important early sign. This is a surgical emergency requiring decompression.
Vascular Supply
The orbit's blood supply comes from the ophthalmic artery — a branch of the internal carotid artery — which enters through the optic canal. Key branches include:
- Central retinal artery — enters the optic nerve 10–12 mm behind the globe
- Posterior ciliary arteries — supply the choroid and optic nerve head
- Anterior ciliary arteries — arise from the extraocular muscle vessels; relevant in strabismus surgery
- Lacrimal artery — supplies the lacrimal gland and lateral upper lid
- Supraorbital and supratrochlear arteries — supply the forehead
Venous drainage is primarily via the superior ophthalmic vein → cavernous sinus. Orbital varix (venous malformation) and carotid-cavernous fistula both affect this system and produce characteristic orbital signs.
Clinical Relevance
Proptosis
Increased orbital volume (fat/tumor/muscle)
See service →Orbital fracture
Thin medial wall or floor (blow-out)
See service →Orbital tumor
Mass within intra- or extraconal space
See service →Optic neuropathy
Apex compression (muscles or tumor)
See service →Enophthalmos
Orbital volume expansion (fracture, atrophy)
See service →Socket reconstruction
Loss of globe (anophthalmos)
See service →Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.